Enfermedad relacionada con inmunoglobulina G4, un diagnóstico a tener en cuenta: a propósito de un caso
DOI:
https://doi.org/10.22516/25007440.978Palabras clave:
Enfermedad relacionada con IgG4, pancreatitis autoinmune, Inmunoglobulina G4Resumen
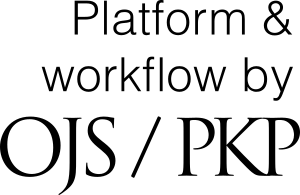
La enfermedad relacionada con inmunoglobulina G4 (ER-IgG4) es una condición inmunomediada y multisistémica asociada al desarrollo de lesiones fibroinflamatorias en cualquier órgano. El diagnóstico se realiza bajo la suma de criterios clínicos, serológicos, radiológicos e histopatológicos; sin embargo, este suele ser difícil debido a su similitud con neoplasias, infecciones u otras enfermedades inmunomediadas. El tratamiento se basa en corticosteroides, en una posible combinación con inmunomoduladores. El presente caso trata de un varón de 59 años con historia de síndrome ictérico y baja de peso, admitido por sospecha de neoplasia maligna de la vía biliar. Las imágenes revelaron estenosis con dilatación de las vías biliares intrahepáticas, páncreas prominente, estenosis del conducto pancreático y lesiones nodulares renales. Debido al antecedente de submandibulectomía izquierda 2 años antes de la enfermedad actual e histología compatible con tumor de Küttner, más los valores elevados de IgG4 sérico, se estableció el diagnóstico de ER-IgG4. Inició tratamiento con corticosteroides y cursó asintomático durante el seguimiento.
Descargas
Referencias bibliográficas
Stone JH, Zen Y, Deshpande V. Mechanisms of disease: IgG4-related disease. N Engl J Med. 2012;366(6):539-51. https://doi.org/10.1056/NEJMRA1104650
Ruiz-Rebollo ML, Álvarez-Quiñones-Sanz M, Fuertes-Alija JJ, Izquierdo-Santervás S. IgG4-related disease mimicking pancreatic tumour. Gastroenterología y Hepatología (English Edition). 2021;44(9):660–1. https://doi.org/10.1016/J.GASTRE.2020.07.026
Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4-related disease. Lancet. 2015;385(9976):1460–71. https://doi.org/10.1016/S0140-6736(14)60720-0
Johnston J, Allen JE. IgG4-related disease in the head and neck. Curr Opin Otolaryngol Head Neck Surg. 2018;26(6):403–8. https://doi.org/10.1097/MOO.0000000000000487
Skillington SA, Ogden MA. IgG4-Related Disease and the Salivary Glands: A Review of Pathophysiology, Diagnosis, and Management. Otolaryngol Clin North Am. 2021;54(3):497–508. https://doi.org/10.1016/J.OTC.2021.02.002
Wallace ZS, Perugino C, Matza M, Deshpande V, Sharma A, Stone JH. IgG4-Related Disease. Clin Chest Med. 2019;40(3):583-97. https://doi.org/10.1016/J.CCM.2019.05.005
Wallace ZS, Naden RP, Chari S, Choi H, Della-Torre E, Dicaire JF, et al. The 2019 American College of Rheumatology/European League Against Rheumatism Classification Criteria for IgG4-Related Disease. Arthritis Rheumatol. 2020;72(1):7–19. https://doi.org/10.1002/ART.41120
Khosroshahi A, Wallace ZS, Crowe JL, Akamizu T, Azumi A, Carruthers MN, et al. International consensus guidance statement on the management and treatment of IgG4-related disease. Arthritis Rheumatol. 2015;67(7):1688–99. https://doi.org/10.1002/ART.39132
Yamamoto M, Yajima H, Takahashi H, Yokoyama Y, Ishigami K, Shimizu Y, et al. Everyday clinical practice in IgG4-related dacryoadenitis and/or sialadenitis: Results from the SMART database. Mod Rheumatol. 2015;25(2):199–204. https://doi.org/10.3109/14397595.2014.950036
Khosroshahi A, Carruthers MN, Deshpande V, Unizony S, Bloch DB, Stone JH. Rituximab for the treatment of IgG4-related disease: Lessons from 10 consecutive patients. Medicine. 2012;91(1):57–66. https://doi.org/10.1097/MD.0B013E3182431EF6
Carruthers MN, Topazian MD, Khosroshahi A, Witzig TE, Wallace ZS, Hart PA, et al. Rituximab for IgG4-related disease: a prospective, open-label trial. Ann Rheum Dis. 2015;74(6):1171–7. https://doi.org/10.1136/ANNRHEUMDIS-2014-206605
Kamisawa T, Funata N, Hayashi Y, Eishi Y, Koike M, Tsuruta K, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol. 2003;38(10):982-4. https://doi.org/10.1007/S00535-003-1175-Y
Uchida K, Masamune A, Shimosegawa T, Okazaki K. Prevalence of IgG4-Related Disease in Japan Based on Nationwide Survey in 2009. Int J Rheumatol. 2012;2012:358371. https://doi.org/10.1155/2012/358371
Masamune A, Kikuta K, Hamada S, Tsuji I, Takeyama Y, Shimosegawa T, et al. Nationwide epidemiological survey of autoimmune pancreatitis in Japan in 2016. J Gastroenterol. 2020;55(4):462-70. https://doi.org/10.1007/S00535-019-01658-7
Wallace ZS, Zhang Y, Perugino CA, Naden R, Choi HK, Stone JH. Clinical phenotypes of IgG4-related disease: an analysis of two international cross-sectional cohorts. Ann Rheum Dis. 2019;78(3):406–12. https://doi.org/10.1136/ANNRHEUMDIS-2018-214603
Zen Y, Nakanuma Y. IgG4-related disease: A cross-sectional study of 114 cases. Am J Surg Pathol, 2010;34(12):1812–9. https://doi.org/10.1097/PAS.0B013E3181F7266B
Pillai S, Perugino C, Kaneko N. Immune mechanisms of fibrosis and inflammation in IgG4-related disease. Curr Opin Rheumatol. 2020;32(2):146–51. https://doi.org/10.1097/BOR.0000000000000686
Della-Torre E, Feeney E, Deshpande V, Mattoo H, Mahajan V, Kulikova M, et al. B-cell depletion attenuates serological biomarkers of fibrosis and myofibroblast activation in IgG4-related disease. Ann Rheum Dis. 2015;74(12):2236. https://doi.org/10.1136/ANNRHEUMDIS-2014-205799
Chen Y, Lin W, Yang H, Wang M, Zhang P, Feng R, et al. Aberrant Expansion and Function of Follicular Helper T Cell Subsets in IgG4-Related Disease. Arthritis Rheumatol. 2018;70(11):1853–65. https://doi.org/10.1002/ART.40556
Furukawa S, Moriyama M, Tanaka A, Maehara T, Tsuboi H, Iizuka M, et al. Preferential M2 macrophages contribute to fibrosis in IgG4-related dacryoadenitis and sialoadenitis, so-called Mikulicz’s disease. Clinical Immunology. 2015;156(1):9–18. https://doi.org/10.1016/J.CLIM.2014.10.008
Lanzillotta M, Lanzillotta M, Mancuso G, Mancuso G, Della-Torre E. Advances in the diagnosis and management of IgG4 related disease. BMJ. 2020;369:m1067. https://doi.org/10.1136/BMJ.M1067
Bhatti RM, Stelow EB. IgG4-related disease of the head and neck. Adv Anat Pathol. 2013;20(1):10–6. https://doi.org/10.1097/PAP.0B013E31827B619E
Mulholland GB, Jeffery CC, Satija P, Côté DWJ. Immunoglobulin G4-related diseases in the head and neck: a systematic review. J Otolaryngol Head Neck Surg.2015;44(1):24. https://doi.org/10.1186/S40463-015-0071-9
Chari ST, Kloeppel G, Zhang L, Notohara K, Lerch MM, Shimosegawa T. Histopathologic and clinical subtypes of autoimmune pancreatitis: The honolulu consensus document. Pancreas. 2010;39(5):549–54. https://doi.org/10.1097/MPA.0B013E3181E4D9E5
Sah RP, Chari ST, Pannala R, Sugumar A, Clain JE, Levy MJ, et al. Differences in Clinical Profile and Relapse Rate of Type 1 Versus Type 2 Autoimmune Pancreatitis. Gastroenterology. 2010;139(1):140–8. https://doi.org/10.1053/J.GASTRO.2010.03.054
Vashi B, Khosroshahi A. IgG4-Related Disease with Emphasis on Its Gastrointestinal Manifestation. Gastroenterol Clin North Am. 2019;48(2):291–305. https://doi.org/10.1016/j.gtc.2019.02.008
Zheng Y, Elsayes KM, Waranch C, Abdelaziz A, Menias CO, Sandrasegaran K, et al. IgG4-related disease in the abdomen and pelvis: atypical findings, pitfalls, and mimics. Abdominal Radiology. 2020;45(8):2485–99. https://doi.org/10.1007/S00261-020-02526-2
Erkelens GW, Vleggaar FP, Lesterhuis W, van Buuren HR, van der Werf SDJ. Sclerosing pancreato-cholangitis responsive to steroid therapy. Lancet. 1999;354(9172):43–4. https://doi.org/10.1016/S0140-6736(99)00603-0
Smal AJ, Loftus CG, Smyrk TC, Baron TH. A case of IgG4-associated cholangitis and autoimmune pancreatitis responsive to corticosteroids. Nat Clin Pract Gastroenterol Hepatol. 2008(12):707–12. https://doi.org/10.1038/NCPGASTHEP1296
Nakazawa T, Ando T, Hayashi K, Naitoh I, Ohara H, Joh T. Diagnostic procedures for IgG4-related sclerosing cholangitis. J Hepatobiliary Pancreat Sci. 2011;18(2):127–36. https://doi.org/10.1007/S00534-010-0320-2
Mendes FD, Jorgensen R, Keach J, Katzmann JA, Smyrk T, Donlinger J, et al. Elevated serum IgG4 concentration in patients with primary sclerosing cholangitis. Am J Gastroenterol. 2006;101(9):2070–5. https://doi.org/10.1111/J.1572-0241.2006.00772.X
Itoi T, Kamisawa T, Igarashi Y, Kawakami H, Yasuda I, Itokawa F, et al. The role of peroral video cholangioscopy in patients with IgG4-related sclerosing cholangitis. Journal of Gastroenterology. 2012;48(4):504–14. https://doi.org/10.1007/S00535-012-0652-6
Saeki T, Ito T, Yamazaki H, Imai N, Nishi S. Hypocomplementemia of unknown etiology: an opportunity to find cases of IgG4-positive multi-organ lymphoproliferative syndrome. Rheumatology International. 2009;30(1):99–103. https://doi.org/10.1007/S00296-009-0925-4
Saeki T, Kawano M, Mizushima I, Yamamoto M, Wada Y, Nakashima H, et al. The clinical course of patients with IgG4-related kidney disease. Kidney Int. 2013;84(4):826–33. https://doi.org/10.1038/KI.2013.191
Carruthers MN, Khosroshahi A, Augustin T, Deshpande V, Stone JH. The diagnostic utility of serum IgG4 concentrations in IgG4-related disease. Ann Rheum Dis. 2015;74(1):14–8. https://doi.org/10.1136/ANNRHEUMDIS-2013-204907
Zhang W, Stone JH. Management of IgG4-related disease. Lancet Rheumatol. 2019;1(1):e55–65. https://doi.org/10.1016/S2665-9913(19)30017-7
Lanzillotta M, Fernàndez-Codina A, Culver E, Ebbo M, Martinez-Valle F, Schleinitz N, et al. Emerging therapy options for IgG4-related disease. Emerging therapy options for IgG4-related disease. Expert Rev Clin Immunol. 2021;17(5):471-83. https://doi.org/10.1080/1744666X.2021.1902310
Okazaki K, Chari ST, Frulloni L, Lerch MM, Kamisawa T, Kawa S, et al. International consensus for the treatment of autoimmune pancreatitis. Pancreatology. 2017;17(1):1–6. https://doi.org/10.1016/J.PAN.2016.12.003
Hart PA, Kamisawa T, Brugge WR, Chung JB, Culver EL, Czakó L, et al. Original article: Long-term outcomes of autoimmune pancreatitis: a multicentre, international analysis. Gut. 2013;62(12):1771. https://doi.org/10.1136/GUTJNL-2012-303617
Omar D, Chen Y, Cong Y, Dong L. Glucocorticoids and steroid sparing medications monotherapies or in combination for IgG4-RD: a systematic review and network meta-analysis. Rheumatology (Oxford). 2020;59(4):718–26. https://doi.org/10.1093/RHEUMATOLOGY/KEZ380
Deshpande V, Zen Y, Chan JKC, Yi EE, Sato Y, Yoshino T, et al. Consensus statement on the pathology of IgG4-related disease. Modern Pathology. 2012;25(9):1181–92. https://doi.org/10.1038/modpathol.2012.72
Descargas
Publicado
Cómo citar
Número
Sección
Licencia
Derechos de autor 2023 Revista colombiana de Gastroenterología

Esta obra está bajo una licencia internacional Creative Commons Atribución-NoComercial-SinDerivadas 4.0.
Aquellos autores/as que tengan publicaciones con esta revista, aceptan los términos siguientes:
Los autores/as ceden sus derechos de autor y garantizarán a la revista el derecho de primera publicación de su obra, el cuál estará simultáneamente sujeto a la Licencia de reconocimiento de Creative Commons que permite a terceros compartir la obra siempre que se indique su autor y su primera publicación en esta revista.
Los contenidos están protegidos bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.

| Estadísticas de artículo | |
|---|---|
| Vistas de resúmenes | |
| Vistas de PDF | |
| Descargas de PDF | |
| Vistas de HTML | |
| Otras vistas | |