Requerimiento de hemostasia endoscópica en pacientes de una unidad de cuidado intensivo con hemorragia de vías digestivas altas
DOI:
https://doi.org/10.22516/25007440.362Palabras clave:
endoscopia, cuidados intensivos, hemorragiaResumen
Introducción: los pacientes hospitalizados en la unidad de cuidados intensivos (UCI) tienen riesgo de hemorragia digestiva alta (HVDA). La endoscopia digestiva alta (EVDA) es el examen de elección en esos pacientes y es diagnóstica y terapéutica. Muchas lesiones identificadas endoscópicamente no requieren tratamiento endoscópico. En Colombia no hay estudios sobre la prevalencia de las diferentes lesiones sangrantes digestivas altas en pacientes de la UCI, ni sobre la utilización de EVDA terapéutica en esos pacientes.
Materiales y métodos: estudio de corte transversal realizado en la Clínica Fundadores de Bogotá, Colombia, entre enero del 2003 a febrero del 2017. Se incluyeron pacientes adultos de la unidad de cuidado intensivo con EVDA indicada por HVDA.
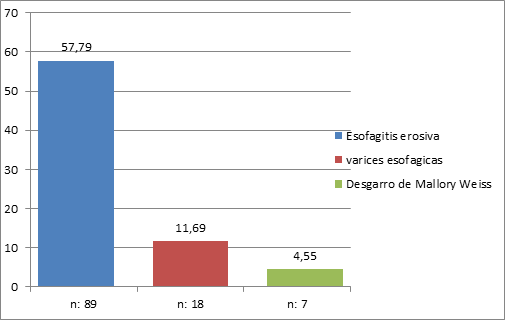
Resultados: en el análisis final se incluyeron 156 EVDA. Los hallazgos fueron los siguientes: gastritis crónica 76,62% (118), esofagitis erosiva (grado A-grado D) 57,79% (89), gastritis erosiva 47,4% (73), duodenitis erosiva 21,43% (33), úlcera gástrica 18,18% (28), varices esofágicas 11,69% (18), úlcera duodenal 11,04% (17) y desgarro de Mallory-Weiss 4,55% (8). Solo el 15% de los pacientes requirió manejo endoscópico, incluidos los que tenían várices esofágicas.
Conclusión: en el presente estudio, el 15% de los pacientes con HVDA requirió tratamiento endoscópico. Se deben realizar trabajos prospectivos que permitan establecer factores de riesgo que puedan predecir la necesidad de EVDA terapéutica en pacientes con HVDA. Quien no tenga esos predictores se debe tratar empíricamente con IBP y evitar gastos innecesarios en EVDA diagnósticas.
Descargas
Referencias bibliográficas
Marik P, Vasu T, Hirani A, Pachinburavan M. Stress ulcer prophylaxis in the new millennium: a systematic review and meta-analysis. Crit Care Med. 2010;38(11):2222-8. doi: https://doi.org/10.1097/CCM.0b013e3181f17adf.
Krag M, Perner A, Wetterslev J, Wise M, Borthwick M, Bendel S, et al. Stress ulcer prophylaxis in the intensive care unit: an international survey of 97 units in 11 countries. Acta Anaesthesiol Scand. 2015;59(5):576-85. doi: https://doi.org/10.1111/aas.12508.
Krag M, Perner A, Wetterslev J, Wise M, Borthwick M, Bendel S, et al. Prevalence and outcome of gastrointestinal bleeding and use of acid suppressants in acutely ill adult intensive care patients. Intensive Care Med. 2015;41(5):833-45. doi: https://doi.org/10.1007/s00134-015-3725-1.
Cook D, Griffith L, Walter S, Guyatt G, Meade M, Heyland DK, et al. The attributable mortality and length of intensive care unit stay of clinically important gastrointestinal bleeding in critically ill patients. Crit Care. 2001;5(6):368. doi: https://doi.org/10.1186/cc1071.
Cook D, Fuller H, Guyatt G, Marshall J, Leasa D, Hall R, et al. Risk factors for gastrointestinal bleeding in critically ill patients. N Engl J Med. 1994;330(6):377-81. doi: https://doi.org/10.1056/NEJM199402103300601.
Cipolletta L, Cipolletta F, Granata A, Ligresti D, Barresi L, Tarantino I, et al. What is the best endoscopic strategy in acute non-variceal gastrointestinal bleeding? Curr Treat Optios Gastro. 2018;16(4):363-75. doi: https://doi.org/10.1007/s11938-018-0192-0.
Jean-Baptiste S, Messika J, Hajage D, Gaudry S, Barbieri J, Duboc H, et al. Clinical impact of upper gastrointestinal endoscopy in critically ill patients with suspected bleeding. Ann Intensive Care. 2018;8(1):75. doi: https://doi.org/10.1186/s13613-018-0423-5.
Barkun A, Bardou M, Kuipers E, Sung J, Hunt R, Martel M, et al. International consensus recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Ann Inter Med. 2010;152(2):101-13. doi: https://doi.org/10.7326/0003-4819-152-2-201001190-00009.
Lau J, Barkun A, Fan DM, Kuipers E, Yang YS, Chan F. Challenges in the management of acute peptic ulcer bleeding. Lancet. 2013;381(9882):2033-43. doi: https://doi.org/10.1016/S0140-6736(13)60596-6.
Chak A, Cooper G, Lloyd L, Kolz C, Barnhart B, Wong R. Effectiveness of endoscopy in patients admitted to the intensive care unit with upper GI hemorrhage. Gastrointest Endoscop. 2001;53(1):6-13. doi: https://doi.org/10.1067/mge.2001.108965.
Lee YC, Wang HP, Wu MS, Yang CS, Chang YT, Lin JT. Urgent bedside endoscopy for clinically significant upper gastrointestinal hemorrhage after admission to the intensive care unit. Intensive Care Med. 2003;29(10):1723-8. doi: https://doi.org/10.1007/s00134-003-1921-x.
Tam W, Bertholini D. Tension pneumoperitoneum, pneumomediastinum, subcutaneous emphysema and cardiorespiratory collapse following gastroscopy. Anaesth Intensive Care. 2007;35(2):307-9.
Conrad SA. Acute upper gastrointestinal bleeding in critically ill patients: causes and treatment modalities. Crit Care Med. 2002;30(6):S365-S8. doi: https://doi.org/10.1097/00003246-200206001-00006.
Eddleston J, Pearson R, Holland J, Tooth J, Vohra A, Doran BH. Prospective endoscopic study of stress erosions and ulcers in critically ill adult patients treated with either sucralfate or placebo. Critic Care Med. 1994;22(12):1949-54. doi: https://doi.org/10.1097/00003246-199422120-00010.
Marker S, Krag M, Møller M. What's new with stress ulcer prophylaxis in the ICU? Intensive Care Med. 2017;43(8):1132-4. doi: https://doi.org/10.1007/s00134-017-4733-0.
Granholm A, Lange T, Anthon C, Marker S, Krag M, Meyhoff T, et al. Timing of onset of gastrointestinal bleeding in the ICU: protocol for a preplanned observational study. Acta Anaesth Scand. 2018. doi: https://doi.org/10.1111/aas.13144.
Plummer M, Blaser A, Deane A. Stress ulceration: prevalence, pathology and association with adverse outcomes. Crit Care. 2014;18(2):213. doi: https://doi.org/10.1186/cc13780.
Steinberg K. Stress-related mucosal disease in the critically ill patient: risk factors and strategies to prevent stress-related bleeding in the intensive care unit. Crit Care Med. 2002;30(6):S362-S4. doi: https://doi.org/10.1097/00003246-200206001-00005.
Siddiqui F, Ahmed M, Abbasi S, Avula A, Siddiqui A, Philipose J, et al. Gastrointestinal bleeding in patients with acute respiratory distress syndrome: a national database analysis. J Clin Med Res. 2019;11(1):42-8. doi: https://doi.org/10.14740/jocmr3660.
Alvarado J. Profilaxis de sangrado digestivo en la Unidad de Cuidados Intensivos. Univ Med. 2002;43(1):33-5.
Schuster D, Rowley H, Feinstein S, McGue M, Zuckerman G. Prospective evaluation of the risk of upper gastrointestinal bleeding after admission to a medical intensive care unit. Am J med. 1984;76(4):623-30. doi: https://doi.org/10.1016/0002-9343(84)90286-9.
Huang HB, Jiang W, Wang CY, Qin HY, Du B. Stress ulcer prophylaxis in intensive care unit patients receiving enteral nutrition: a systematic review and meta-analysis. Crit Care. 2018;22(1):20. doi: https://doi.org/10.1186/s13054-017-1937-1.
Beejay U, Wolfe M. Acute gastrointestinal bleeding in the intensive care unit: the gastroenterologist's perspective. Gastroenterol Clin North Am. 2000;29(2):309-36. doi: https://doi.org/10.1016/S0889-8553(05)70118-7.
Morales C, Sierra S, Hernández A, Arango A, López G. Hemorragia digestiva alta: factores de riesgo para mortalidad en dos centros urbanos de América Latina. Rev Esp Enferme Dig. 2011;103(1):20-4. doi: https://doi.org/10.4321/S1130-01082011000100004.
Lewis J, Shin E, Metz D. Characterization of gastrointestinal bleeding in severely ill hospitalized patients. Crit Care Med. 2000;28(1):46-50. doi: https://doi.org/10.1097/00003246-200001000-00007.
Kim J, Kim J, Chun J, Lee C, Im J, Kim J. Early versus late bedside endoscopy for gastrointestinal bleeding in critically ill patients. Korean J Intern med. 2018;33(2):304-12. doi: 10.3904/kjim.2016.182.
Hayden S, Albert T, Watkins T, Swenson E. Anemia in critical illness: insights into etiology, consequences, and management. American J Respir Crit Care Med. 2012;185(10):1049-57. doi: https://doi.org/10.1164/rccm.201110-1915CI.
Sesler J. Stress-related mucosal disease in the intensive care unit. AACN Advanced Crit Care. 2007;18(2):119-28. doi: https://doi.org/10.4037/15597768-2007-2004.
Silverstein F, Gilbert D, Tedesco F, Buenger N, Persing J. The national ASGE survey on upper gastrointestinal bleeding: II. Clinical prognostic factors. Gastrointest Endoscop. 1981;27(2):80-93. doi: https://doi.org/10.1016/S0016-5107(81)73156-0.
van Leerdam M. Epidemiology of acute upper gastrointestinal bleeding. Best Pract Res Clin Gastroenterol. 2008;22(2):209-24. doi: https://doi.org/10.1016/j.bpg.2007.10.011.
Ovenden C, Plummer M, Selvanderan S, Donaldson T, Nguyen N, Weinel L, et al. Occult upper gastrointestinal mucosal abnormalities in critically ill patients. Acta Anaesthesiol Scand. 2017;61(2):216-23. doi: https://doi.org/10.1111/aas.12844.
Rich K. Overview of Mallory-Weiss syndrome. J Vasc Nurs. 2018;36(2):91-3. doi: https://doi.org/10.1016/j.jvn.2018.04.001.
Guelrud M. Mallory-Weiss syndrome. UptoDate. 2017. Último acceso: 15 de junio de 2018. Disponible en: https://www.uptodate.com/contents/mallory-weiss-syndrome
Cucci M, Capputo F, Fraternali G, Roncallo A, Ventura F. Transition of a Mallory-Weiss syndrome to a Boerhaave syndrome confirmed by anamnestic, necroscopic, and autopsy data. A case report. Medicine (Baltimore). 2018;97(49):e13191. doi: https://doi.org/10.1097/MD.0000000000013191.
Skok P, Sinkovič A. Upper gastrointestinal haemorrhage: predictive factors of in-hospital mortality in patients treated in the medical intensive care unit. J Int Med Res. 2011;39(3):1016-27. doi: https://doi.org/10.1177/147323001103900337.
Gralnek I, Dumonceau J, Kuipers E, Lanas A, Sanders D, Kurien M, et al. Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2015;47(10):a1-a46. doi: https://doi.org/10.1055/s-0034-1393172.
Krag M, Marker S, Perner A, Wetterslev J, Wise M, Schefold J, et al. Pantoprazole in patients at risk for gastrointestinal bleeding in the ICU. N Engl J Med. 2018;379(23):2199-208.
Rehman A, Iscimen R, Yilmaz M, Khan H, Belsher J, Gomez JF, et al. Prophylactic endotracheal intubation in critically ill patients undergoing endoscopy for upper GI hemorrhage. Gastrointest Endoscop. 2009;69(7):e55-e9. doi: https://doi.org/10.1016/j.gie.2009.03.002.
Descargas
Publicado
Cómo citar
Número
Sección
Licencia
Aquellos autores/as que tengan publicaciones con esta revista, aceptan los términos siguientes:
Los autores/as ceden sus derechos de autor y garantizarán a la revista el derecho de primera publicación de su obra, el cuál estará simultáneamente sujeto a la Licencia de reconocimiento de Creative Commons que permite a terceros compartir la obra siempre que se indique su autor y su primera publicación en esta revista.
Los contenidos están protegidos bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.

| Estadísticas de artículo | |
|---|---|
| Vistas de resúmenes | |
| Vistas de PDF | |
| Descargas de PDF | |
| Vistas de HTML | |
| Otras vistas | |