Utilidad de la plasmaféresis en la pancreatitis aguda por hipertrigliceridemia
A propósito de un caso
DOI:
https://doi.org/10.22516/25007440.350Palabras clave:
Pancreatitis, hipertrigliceridemia, plasmaféresis.Resumen
Introducción: la pancreatitis aguda es una entidad de alta incidencia e impacto a nivel mundial. Presenta múltiples causas dentro de las cuales las más frecuentes son la obstrucción de la vía biliar, el consumo de alcohol y, en tercer orden, la hipertrigliceridemia. Esta última se entiende como aquellos niveles séricos de triglicéridos >1000 mg/dL. Dicho escenario representa entre el 1 y el 7 % del total de los casos.
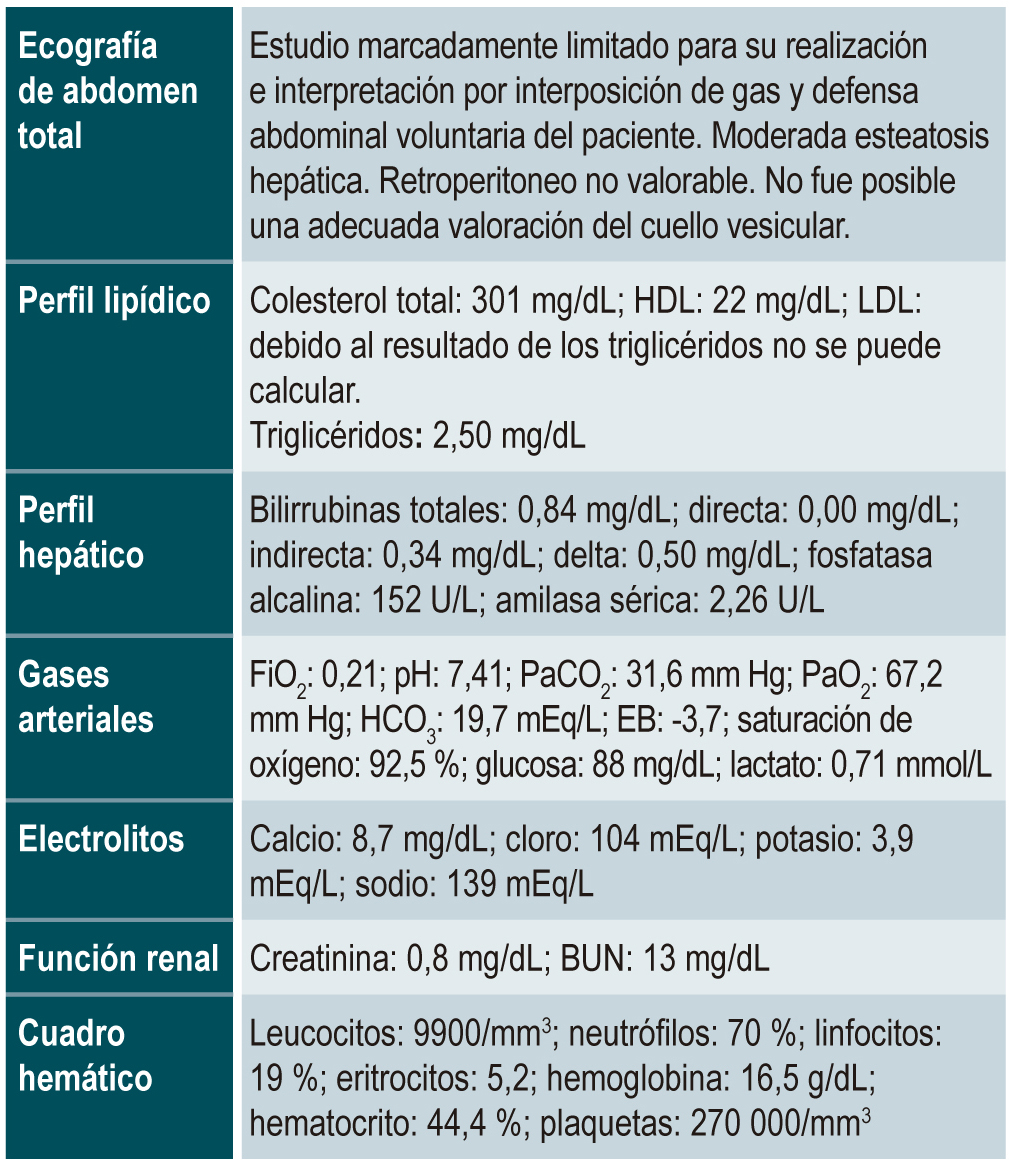
Metodología: presentamos un caso de pancreatitis aguda secundaria a hipertrigliceridemia severa, manejada con plasmaféresis. Se realiza una revisión de la literatura sobre las condiciones, indicaciones y ventajas de esta estrategia terapéutica.
Conclusiones: en casos escogidos, la plasmaféresis es una estrategia de manejo segura y efectiva en el tratamiento de pacientes con pancreatitis aguda secundaria a hipertrigliceridemia severa.
Descargas
Referencias bibliográficas
Brisinda G, Vanella S, Crocco A, Mazzari A, Tomaiuolo P, Santullo F, Grossi U, Crucitti A. Severe acute pancreatitis: advances and insights in assessment of severity and management. Eur J Gastroenterol Hepatol. 2011;23(7):541‐551. http://doi.org/10.1097/MEG.0b013e328346e21e
Bae JH, Baek SH, Choi HS, Cho KR, Lee HL, Lee OY, Yoon BC, Hahm JS, Lee MH, Lee DH, Kee CS. Acute pancreatitis due to hypertriglyceridemia: report of 2 cases. Korean J Gastroenterol. 2005;46(6):475‐480.
Whitcomb DC. Genetic aspects of pancreatitis. Annu Rev Med. 2010;61:413‐424.
http://doi.org/10.1146/annurev.med.041608.121416
Fujita K, Maeda N, Kozawa J, Murano K, Okita K, Iwahashi H, Kihara S, Ishigami M, Omura M, Nakamura T, Shirai K, Yamamura T, Funahashi T, Shimomura I. A case of adolescent hyperlipoproteinemia with xanthoma and acute pancreatitis, associated with decreased activities of lipoprotein lipase and hepatic triglyceride lipase. Intern Med. 2010;49(22):2467‐2472.
http://doi.org/10.2169/internalmedicine.49.4058
Dominguez-Muñoz JE, Malfertheiner P, Ditschuneit HH, Blanco-Chavez J, Uhl W, Büchler M, Ditschuneit H. Hyperlipidemia in acute pancreatitis. Relationship with etiology, onset, and severity of the disease. Int J Pancreatol. 1991;10(3-4):261‐267.
Olofsson SO, Borèn J. Apolipoprotein B: a clinically important apolipoprotein which assembles atherogenic lipoproteins and promotes the development of atherosclerosis. J Intern Med. 2005;258(5):395‐410.
http://doi.org/10.1111/j.1365-2796.2005.01556.x
Packard CJ, Shepherd J. Lipoprotein heterogeneity and apolipoprotein B metabolism. Arterioscler Thromb Vasc Biol. 1997;17(12):3542‐3556.
http://doi.org/10.1161/01.atv.17.12.3542
Iqbal J, Hussain MM. Intestinal lipid absorption. Am J Physiol Endocrinol Metab. 2009;296(6):E1183‐E1194. http.//doi.org/10.1152/ajpendo.90899.2008
Criddle DN, Raraty MG, Neoptolemos JP, Tepikin AV, Petersen OH, Sutton R. Ethanol toxicity in pancreatic acinar cells: mediation by nonoxidative fatty acid metabolites. Proc Natl Acad Sci U S A. 2004;101(29):10738‐10743. http://doi.org/10.1073/pnas.0403431101
Sakorafas GH, Tsiotou AG. Etiology and pathogenesis of acute pancreatitis: current concepts. J Clin Gastroenterol. 2000;30(4):343‐356.
http://doi.org/10.1097/00004836-200006000-00002
Kolovou GD, Anagnostopoulou KK, Kostakou PM, Bilianou H, Mikhailidis DP. Primary and secondary hypertriglyceridaemia. Curr Drug Targets. 2009;10(4):336‐343. http://doi.org/10.2174/138945009787846452
Karabatas L, Oliva ME, Dascal E, Hein GJ, Pastorale C, Chicco A, Lombardo YB, Basabe JC. Is Lipotoxicity presents in the early stages of an experimental model of autoimmune diabetes? Further studies in the multiple low dose of streptozotocin model. Islets. 2010;2(3):190‐199. http://doi.org/10.4161/isl.2.3.11655
Apte MV, Wilson JS. Alcohol-induced pancreatic injury. Best Pract Res Clin Gastroenterol. 2003;17(4):593‐612. http://doi.org/10.1016/s1521-6918(03)00050-7
Elisaf MS, Nakou K, Liamis G, Pavlidis NA. Tamoxifen-induced severe hypertriglyceridemia and pancreatitis. Ann Oncol. 2000;11(8):1067‐1069.
http://doi.org/10.1023/a:1008309613082
Bildirici I, Esinler I, Deren O, Durukan T, Kabay B, Onderoglu L. Hyperlipidemic pancreatitis during pregnancy. Acta Obstet Gynecol Scand. 2002;81(5):468‐470. http://doi.org/10.1034/j.1600-0412.2002.810516.x
Kadikoylu G, Yukselen V, Yavasoglu I, Coşkun A, Karaoglu AO, Bolaman Z. Emergent therapy with therapeutic plasma exchange in acute recurrent pancreatitis due to severe hypertriglyceridemia. Transfus Apher Sci. 2010;43(3):285‐289.
http://doi.org/10.1016/j.transci.2010.09.009
Lawson EB, Gottschalk M, Schiff DE. Insulin infusion to treat severe hypertriglyceridemia associated with pegaspargase therapy: a case report. J Pediatr Hematol Oncol. 2011;33(2):e83‐e86.
http://doi.org/10.1097/MPH.0b013e3181f46c22
Pavlic M, Xiao C, Szeto L, Patterson BW, Lewis GF. Insulin acutely inhibits intestinal lipoprotein secretion in humans in part by suppressing plasma free fatty acids. Diabetes. 2010;59(3):580‐587.
http://doi.org/10.2337/db09-1297
Mikhail N, Trivedi K, Page C, Wali S, Cope D. Treatment of severe hypertriglyceridemia in nondiabetic patients with insulin. Am J Emerg Med. 2005;23(3):415‐417.
http://doi.org/10.1016/j.ajem.2005.02.036
Cole RP. Heparin treatment for severe hypertriglyceridemia in diabetic ketoacidosis. Arch Intern Med. 2009;169(15):1439‐1441.
http://doi.org/10.1001/archinternmed.2009.221
Patel YC. Somatostatin and its receptor family. Front Neuroendocrinol. 1999;20(3):157‐198.
http://doi.org/10.1006/frne.1999.0183
Taniyama Y, Suzuki T, Mikami Y, Moriya T, Satomi S, Sasano H. Systemic distribution of somatostatin receptor subtypes in human: an immunohistochemical study. Endocr J. 2005;52(5):605‐611.
http://doi.org/10.1507/endocrj.52.605
Ewald N, Kloer HU. Severe hypertriglyceridemia: an indication for apheresis? Atheroscler Suppl. 2009;10(5):49‐52. http://doi.org/10.1016/S1567-5688(09)71810-0
Yeh JH, Chen JH, Chiu HC. Plasmapheresis for hyperlipidemic pancreatitis. J Clin Apher. 2003;18(4):181‐185. http://doi.org/10.1002/jca.10063
Syed H, Bilusic M, Rhondla C, Tavaria A. Plasmapheresis in the treatment of hypertriglyceridemia-induced pancreatitis: A community hospital’s experience. J Clin Apher. 2010;25(4):229‐234.
http://doi.org/10.1002/jca.20232
Schwartz J, Padmanabhan A, Aqui N, Balogun RA, Connelly-Smith L, Delaney M, Dunbar NM, Witt V, Wu Y, Shaz BH. Guidelines on the use of therapeutic apheresis in clinical practice—Evidence‐based approach from the apheresis applications committee of the American society for apheresis. J Clin Apher. 2007;22(3):106‐175.
https://doi.org/10.1002/jca.20129
Seda G, Meyer JM, Amundson DE, Daheshia M. Plasmapheresis in the management of severe hypertriglyceridemia. Crit Care Nurse. 2013;33(4):18‐24.
http://doi.org/10.4037/ccn2013346
Keech A, Simes RJ, Barter P, Best J, Scott R, Taskinen MR, Forder P, Pillai A, Davis T, Glasziou P, Drury P, Kesäniemi YA, Sullivan D, Hunt D, Colman P, d’Emden M, Whiting M, Ehnholm C, Laakso M; FIELD study investigators. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet. 2005;366(9500):1849‐1861.
http://doi.org/10.1016/S0140-6736(05)67667-2
Brown BG, Zhao XQ, Chait A, Fisher LD, Cheung MC, Morse JS, Dowdy AA, Marino EK, Bolson EL, Alaupovic P, Frohlich J, Albers JJ. Simvastatin and niacin, antioxidant vitamins, or the combination for the prevention of coronary disease. N Engl J Med. 2001;345(22):1583‐1592. http://doi.org/10.1056/NEJMoa011090
Hu FB, Bronner L, Willett WC, Stampfer MJ, Rexrode KM, Albert CM, Hunter D, Manson JE. Fish and omega-3 fatty acid intake and risk of coronary heart disease in women. JAMA. 2002;287(14):1815‐1821.
http://doi.org/10.1001/jama.287.14.1815
Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto miocardico. Lancet. 1999;354(9177):447‐455.
https://doi.org/10.1016/S0140-6736(99)07072-5
Tsuang W, Navaneethan U, Ruiz L, Palascak JB, Gelrud A. Hypertriglyceridemic pancreatitis: presentation and management. Am J Gastroenterol. 2009;104(4):984‐991. http://doi.org/10.1038/ajg.2009.27
Descargas
Publicado
Cómo citar
Número
Sección
Licencia
Aquellos autores/as que tengan publicaciones con esta revista, aceptan los términos siguientes:
Los autores/as ceden sus derechos de autor y garantizarán a la revista el derecho de primera publicación de su obra, el cuál estará simultáneamente sujeto a la Licencia de reconocimiento de Creative Commons que permite a terceros compartir la obra siempre que se indique su autor y su primera publicación en esta revista.
Los contenidos están protegidos bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.

| Estadísticas de artículo | |
|---|---|
| Vistas de resúmenes | |
| Vistas de PDF | |
| Descargas de PDF | |
| Vistas de HTML | |
| Otras vistas | |